
|
Products Related to Zika, WestNile, Dengue, Malaria, T.B, Chikungunya, HIV, SARS |
|
Product# 15007: Recombinant Treponema pallidum 47kD Membrane Protein (E.coli) |
|
Product# 15009: Recombinant Treponema pallidum TmpA Membrane Protein (E.coli) |
|
Product# 15005: Recombinant Treponema pallidum 17kD Membrane Protein (E.coli) |
Abstract
Multiple concurrent infectious processes have previously been reported in the context of advanced HIV with significant immunosuppression. Here we report a case of multiple infections in a 56-year-old man with well-controlled HIV diagnosed 5 years earlier. Soon after returning to Australia following 12 years living in Thailand, he became unwell with fevers, night sweats, arthralgia and myalgia. There were no localising symptoms and examination was unremarkable. Investigations revealed positive syphilis (Treponema pallidum) serology with an RPR of 16, a positive urine culture (Klebsiella pneumoniae), a pulmonary nodule, a liver abscess and colitis (Entamoeba histolytica). Recovery was only complete when all the individual infections were treated.
Background
According to the principle of parsimony, a single explanation should be sought for a patient’s symptoms, but sometimes the truth is more complex.1 2 Non-specific symptoms such as fever have a wide range of differential diagnoses in patients with HIV, even when infection is well controlled and the CD4 T-cell count is robust. Here, we describe a case of a previously well HIV-positive man with good immune preservation, who was concurrently infected with Treponema pallidum, Klebsiella pneumoniae and Entamoeba histolytica. This complex case demonstrates the importance of consideration of multiple aetiologies and continued investigation where symptoms persist despite an initial diagnosis and appropriate management.
Case presentation
First visit
In late 2013, a 56-year-old Caucasian Australian man presented for HIV care. He stated that he was well and only wanted a supply of his HIV antiretrovirals. He had been diagnosed with HIV-1 in Thailand in 2008 and this was well managed with oral tenofovir (300 mg), emtricitabine (200 mg) and efavirenz (600 mg) daily, commenced at diagnosis. He had a history of syphilis treated within the past 2 years, an appendicectomy in 1987, haemorrhoids and an ulcerative perianal condition for which he had surgery. Approximately 2 months before this presentation, he had returned to Australia after living in Bangkok for 12 years. He preferred male sexual partners and did not have a regular partner at the time. He was seeking a new job in Australia and was well supported by a local family. Antiretrovirals were his only regular medications. He was an ex-smoker, having quit 2 months earlier. He rarely drank alcohol and did not use any recreational drugs.
A script for coformulated tenofovir, emtricitabine and efavirenz was provided, and he was offered standard HIV care and sexually transmissible infection screening. He deferred chlamydia and gonorrhea screening to a later date. HIV testing confirmed the diagnosis of HIV with an undetectable HIV viral load (<20 copies/mL). He had a robust CD4 count (750×106 cells/mL). Full blood count revealed an elevated white cell count of 18.4×109 cells/L, with neutrophilia of 13.3×109 cells/L. He had normal liver, kidney and thyroid function; lipid profile and bone studies. Hepatitis A IgG was detected, confirming immunity. Hepatitis B surface antibody was detected, while surface antigen and core antibody were not detected, consistent with immunity from vaccination. Hepatitis C serology was negative. Syphilis serology was positive with reactive Rapid Plasma Reagin (RPR; titre 16), Venereal Disease Research Laboratory (VDRL; titre 16), Treponema Pallidum Particle Agglutination assay (TPPA) and Fluorescent Treponemal Antibody Absorption Test (FTA-Abs) reactive, consistent with current infection.
Day 2: treatment for syphilis
On recall for syphilis treatment, he revealed that he had been told 3 months ago that he had possibly been exposed to syphilis and had not yet sought testing or treatment. He stated that over the past 4 days he had experienced headache, fatigue, myalgia and an episode of night sweats. This had been preceded by a few days of frequent, loose stools without urgency, blood or mucus, which was now resolved. He denied any ulcers or sores, rash, cough, recent unintended weight loss or recent insect/animal exposures. Neurological examination was normal, with no focal changes to suggest neurosyphilis. He was diagnosed with early syphilis and treated with imtramuscular benzathine penicillin (1.8 g=2 400 000 IU).
Day 11: ongoing symptoms, a positive urine culture and a pulmonary nodule
On review shortly after the syphilis treatment, he reported ongoing night sweats, chills, myalgia and fatigue. On re-examination he was afebrile and normotensive with heart rate 72 beats per minute. His body mass index was 22 kg/m2. He had a few pink papules on the anterior chest. Ear, nose and throat examination was normal. There were no hand signs, and no cervical or axillary lymphadenopathy. Heart sounds were dual without murmur, the chest was clear and the abdomen was soft and non-tender with no organomegaly or palpable masses. Neurological examination was unremarkable. Haematinics, renal and liver function, creatine kinase, serology for Toxoplasma, cytomegatovirus and Epstein-Barr virus, urine microscopy culture and sensitivities, and a chest radiograph were ordered. He declined an offer of admission for further investigations and treatment, but agreed to referral to the thoracic clinic for tuberculosis testing.
His white cell count remained elevated (18.3×109 cells/L, neutrophils 14.1×109 cells/L) as was his C reactive protein at 56.2 mg/L. Urine culture was reported positive for K. pneumoniae (sensitive to amoxicillin with clavulanic acid, cephalexin, gentamicin and trimethoprim and resistant to ampicillin and nitrofurantoin). He had serological evidence of previous exposure to Toxoplasma, CMV and EBV. Chlamydia and gonorrhea screening tests (nucleic acid amplification testing) of the urine, pharynx and rectum were negative. Given the positive urine results, he was started on oral trimethoprim 300 mg nocte for 10 days for suspected pyelonephritis.
The chest X-ray revealed a 1 cm left perihilar nodule. CT scans of the chest, abdomen and pelvis were ordered to further assess the chest lesion and to investigate the possibility of an infectious collection, haematological or other malignancy, tuberculosis or other cause of fevers.
Subsequent Mantoux testing and interferon gamma release assay were negative. A series of three blood cultures, a mycoplasma blood culture, three sputum cultures and three acid-fast stains were also negative.
Day 22: lung and liver lesions
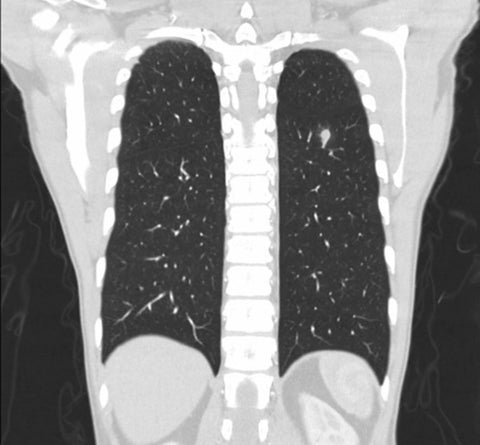
Despite normalisation of his C reactive protein after the treatment with trimethoprim, the patient remained unwell, with ongoing fevers. CT of chest/abdomen/pelvis revealed a 0.9 cm spiculated left lung lesion and a 4.4×3.5×4 cm lesion in segment 3 of the liver, possibly involving the adjacent area of the stomach (figures 1 and 2). No other abnormalities were identified. To further characterise the liver abscess and guide treatment, fine-needle aspiration, serum alpha-fetoprotein and lactate dehydrogenase, coagulation studies and serology for Entamoeba and Strongyloides were ordered. Microscopy of the abscess fluid showed only inflammatory material, with no growth after 3 days of culture.
Open in a separate window
Figure 1
Chest CT of a 56-year-old HIV-positive man with fevers and night sweats demonstrating a 1 cm perihilar nodule.

Figure 2
Abdominal CT scan of a 56-year-old HIV-positive man with fevers and night sweats demonstrating a 4.4×3.5×4 cm liver abscess.
His treatment was changed to cephalexin 1 g four times a day for 3 months for suspected disseminated K. pneumoniae infection which led to further improvement, but not complete resolution, of his symptoms.
1–3 months: positive FOBT and Entamoeba serology
At this point, a faecal occult blood test (FOBT) done as part of standard colorectal cancer screening was reported as showing one negative result and one positive. His Entamoeba serology was positive (titre 2560) with no change on repeat testing 6 weeks later. Strongyloides serology was negative. Three consecutive stool samples demonstrated normal flora only and were negative for cysts or trophozoites. The patient declined colonoscopy, any other investigations or any further antibiotics, at this stage. He was increasingly concerned about the impact of antibiotics of his gastrointestinal flora and developed a depressed mood. This was addressed with psychotherapy, and a trial of Selective Seratonin Reuptake Inhibitors and Seratonin and Noradrenalin Reuptake Inhibitors, neither of which he tolerated. Repeat syphilis serology showed a twofold drop in RPR by 3 months post-treatment, consistent with effective treatment.
4–6 months: ongoing fevers and new gastrointestinal symptoms
Having completed courses of benzathine penicillin, trimethoprim and cephalexin, with normalisation of his RPR, C reactive protein and white cell count, he reported ongoing fatigue and night sweats in addition to new-onset abdominal bloating with intermittent constipation and diarrhoea. A little over a month later, he agreed to be referred for further imaging and colonoscopy.
Repeat CT of chest/abdomen/pelvis showed almost complete resolution of the liver lesion and a reduction in size of the lung lesion, but a new 1.1×1.8 cm rim-enhancing region in the caecal pole.
7 months: amoebic colitis
Colonoscopy confirmed active colitis with multiple ulcers up to 5 mm in size, positive for Entamoeba on histology (figure 3). The treatment was initiated with metronidazole 400 mg three times per day for 2 weeks followed by a course of paromomycin 500 mg TDST for 7 days. Post-treatment stool samples for microscopy, culture and sensitivities and parasitology screen were negative.

Figure 3
Colon biopsy histology specimen from a 56-year-old HIV-positive man with fevers and night sweats demonstrating colitis and Entamoeba spp.
Go to:
Outcome and follow-up
The symptoms of fever and night sweats fully resolved after the treatment for E. histolytica. It took a further of 12–18 months for symptoms of intermittent bloating, diarrhoea and constipation to settle, and for his depression to resolve.
Go to:
Discussion
We have described a patient whose seemingly simple symptom complex of fever, myalgia and night sweats reflected both multisite infection (urinary tract, colon, liver, lung and systemic) and multiple infectious agents (T. pallidum, E. histolytica and K. pneumoniae). This contradicts the widely accepted principle of parsimony in medicine. Why would a multisite, multiagent infection occur in a man in his 50s without substantial immune suppression? The answer partly lies in the shared risk factors of international travel, HIV and male to male sex.
Principle of parsimony
William of Occam’s argument ‘pluralitus non est ponenda sine necessitate’, that explanations should be no more complicated than necessary, has been interpreted in medicine as recommending a single diagnosis to cover a patient’s symptoms and use of the simplest possible pharmacological intervention,1 but this approach has been challenged in the context of contemporary learning theory.2 While a single diagnosis is capable of manifesting a complex range of symptoms, it must be considered that comorbidities are common, and multiple common diseases may be more likely than a single very rare one. Furthermore, some diseases are more likely to co-occur due to shared risk factors.
Causes of fever
The causes of fever are broad and can pose a particular challenge in the context of international travel and HIV infection. Looking at the region of the world where this man had been living, a prospective study of HIV-positive patients presenting with fever to a tertiary hospital in Thailand3 found 85% to be of infectious aetiology, most commonly tuberculosis. A quarter had multiple aetiologies, most commonly tuberculosis and a second or third agent. A study of febrile illness in patients with HIV attending a hospital emergency department in Taiwan4 found lower respiratory tract infections to be the most common cause at 34.7%, with Pneumocystis jirovecii as one of the most commonly identified pathogens. Skin and soft tissue infections were the second most common cause of fever (15.8%) and Staphylococcus aureus skin and soft-tissue infections were more common in those with higher lymphocyte counts. Intra-abdominal and urinary tract infections were also common (11.2% and 6.7%, respectively). In both of these studies, the patients had low CD4 counts, unlike the case presented here. How do causes of fever differ in the general southeast Asian patient population?
A prospective study of hospital presentations for fever in southern India in 20075 found tuberculosis, lower respiratory tract infection and urinary tract infection to be the most common infectious causes. Fifteen per cent had a non-infectious cause of fever and 13% did not receive a diagnosis. Two per cent were diagnosed with amoebic liver abscess.
Causes of liver and pulmonary abscess
Our patient was found to have both liver and pulmonary abscesses. A retrospective file review from Thailand, looking at causative agents of liver abscess in HIV-positive patients over a 10-year period,6 found Mycobacterium tuberculosis, K. pneumoniae and E. histolytica all to be common causes (22%, 17% and 17% of cases, respectively), with pyogenic abscess from any cause far exceeding amoebic liver abscess in prevalence. The symptoms of pyogenic versus amoebic abscess were comparable, and HIV-positive patients did not present differently to patients without HIV.7
While amoebic pulmonary abscess has been described8–10 it is not common. However, it has been suggested that HIV-positive individuals may be more susceptible to invasive amoebic disease.11 In contrast, K. pneumoniae is the most common cause of community-acquired lung abscess in Taiwan12 and is an emerging cause of disease in Asia generally.13 Invasive K. pneumoniae disease has been widely described in recent years, including in Thailand, with infection reported at hepatic, pulmonary, cerebral, renal and ophthalmic sites, including multisite infection and blood stream infection.14–16 Syphilis has also been identified as a cause of multisite infection in the context of HIV in Thailand, with concurrent lung and brain lesions reported in an HIV-positive Thai man diagnosed with syphilis (the brain lesion, but not the lung lesion was confirmed as T. pallidum on PCR testing).17
So, fever may have multiple causes, as may pulmonary, liver and other collections. K. pneumoniae, E. histolytica and T. pallidum are all important causes of febrile illness in southeast Asia, and people with significant immunosuppression are at a risk of multiple infections.
Multiple infection
Previous publications have described multiple concurrent diagnoses in the context of HIV in patients with low or very low CD4 counts, or in people who are severely immunosuppressed for other reasons. Shah et al18 described a presentation of fevers, night sweats, diarrhoea, anorexia and weight loss in a patient with HIV with a CD4 count of 0.003×106 cells/mL (2%) that was found to reflect simultaneous disseminated histoplasmosis, pneumocystis and candidiasis.18 Saha reported simultaneous diagnoses of HIV, Toxoplasma gondii, M. tuberculosis and Cryptococcus neoformans in an Indian man with a CD4 count of 0.152×106 cells/mL, including a multimicrobial (M. tuberculosis and C. neoformans) brain abscess.19 Silber et al20 reported concurrent C. neoformans and M. tuberculosis, and C. neoformans and neurosyphilis in patients with HIV.20 Kitkungvan et al3 reported mixed infectious aetiology in 25% of HIV positive patients with an infectious cause of fever3 at their hospital in Thailand.
The case we present, however, was not one of profound immunosuppression. The patient had been taking HIV antiretrovirals since his initial diagnosis and reported a consistent CD4 count in the range of 800×106 cells/mL, confirmed as 750×106 cells/mL at the time of this illness. He was an international traveller, living with HIV, who had male sexual partners. These factors can act as both individual and shared risks.
Shared risk factors and multiple aetiologies
HIV,21 syphilis,21 E. histolytica22 23 and invasive K. pneumoniae13 15 are all relatively common in Thailand and other southeast Asian countries. Syphilis is positively associated with HIV in Thai sexually transmitted disease clinic attendees.24 HIV,25 syphilis26 and E. histolytica22 are more common in men who have male sexual partners. An Iranian study found a positive association between HIV positivity and positive E. histolytica serology regardless of CD4 count,27 which may reflect an increased risk of HIV infection through damaged rectal mucosa in the case of Entamoeba colitis. Invasive amoebiasis has been reported increasingly in men who have male sexual partners with HIV in southeast Asia, and invasive amoebiasis has also been found to be associated with both syphilis and HIV infection in Japan.22
Go to:
Conclusion
The principle of parsimony is not always right: even apparently simple medical presentations can have multiple simultaneous aetiologies. In some cases, this may reflect shared risk factors, but it can also simply be a co-occurrence of common conditions. The patients do not have to have significant immunocompromise to have multiple infections.
Patients’s perspective
I am very grateful for the range of support provided to me. For me, the greatest impact has been and continues to be depression. Initially that associated with hypoglycaemia while my organs were affected and subsequently that due to degradation of my gut microbiota after 6 contiguous months of antibiotics.
Learning points
- Fever has many causes, and multiple simultaneous infections should be considered if symptoms do not fully resolve after initial diagnosis and treatment.
- When considering coinfection, attention should be given to shared risk factors such as travel and sexual exposures.
- Klebsiella pneumoniae and Entamoeba histolytica are important causes of liver abscess and disseminated disease in southeast Asia.
- HIV, syphilis and E. histolytica are all the more common in men who have male sexual partners.
Go to:
Footnotes
Contributors: MS: conceived the idea for this publication, reviewed the patient file, carried out appropriate literature review and drafted the paper. SJM: reviewed and discussed the patient file, provided feedback on the initial manuscript and approved the final version.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
Go to:
References
- Kalra S, Gupta Y, Sahay R. The law of therapeutic parsimony. Indian J Endocrinol Metab 2016;20:283–4. 10.4103/2230-8210.180008 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Bleakley A. Blunting Occam’s razor: aligning medical education with studies of complexity. J Eval Clin Pract 2010;16:849–55. 10.1111/j.1365-2753.2010.01498.x [PubMed] [CrossRef] [Google Scholar]
- Kitkungvan D, Apisarnthanarak A, Plengpart P, et al. . Fever of unknown origin in patients with HIV infection in Thailand: an observational study and review of the literature. Int J STD AIDS 2008;19:232–5. 10.1258/ijsa.2007.007191 [PubMed] [CrossRef] [Google Scholar]
- Lee CC, Hsieh CC, Chan TY, et al. . Community-onset febrile illness in HIV-infected adults: variable pathogens in terms of CD4 counts and transmission routes. Am J Emerg Med 2015;33:80–7. 10.1016/j.ajem.2014.10.013 [PubMed] [CrossRef] [Google Scholar]
- Abrahamsen SK, Haugen CN, Rupali P, et al. . Fever in the tropics: aetiology and case-fatality – a prospective observational study in a tertiary care hospital in South India. BMC Infect Dis 2013;30:355–62. [PMC free article] [PubMed] [Google Scholar]
- Wiwanitkit V. Causative agents of liver abscess in HIV-seropositive patients: a 10-year case series in Thai hospitalized patients. Trop Doct 2005;35:115–7. 10.1258/0049475054036904 [PubMed] [CrossRef] [Google Scholar]
- Wiwanitkit V. A note on clinical presentations of amebic liver abscess: an overview from 62 Thai patients. BMC Fam Pract 2002;3:13 10.1186/1471-2296-3-13 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Teramoto K, Yamashita N, Kuwabara M, et al. . An amebic lung abscess: report of a case. Surg Today 2001;31:820–2. 10.1007/s005950170056 [PubMed] [CrossRef] [Google Scholar]
- Hugard L, Dubrous P, Massoure PL, et al. . Amebic lung abscess: an unexpected diagnosis. Bull Soc Pathol Exot 2005;98:89–90. [PubMed] [Google Scholar]
- Lichtenstein A, Kondo AT, Visvesvara GS, et al. . Pulmonary amoebiasis presenting as superior vena cava syndrome. Thorax 2005;60:350–2. 10.1136/thx.2004.021014 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis. Clin Chest Med 2002;23:479–92. 10.1016/S0272-5231(01)00008-9 [PubMed] [CrossRef] [Google Scholar]
- Wang JL, Chen KY, Fang CT, et al. . Changing bacteriology of adult community-acquired lung abscess in Taiwan: Klebsiella pneumoniaeversus anaerobes. Clin Infect Dis 2005;40:915–22. 10.1086/428574 [PubMed] [CrossRef] [Google Scholar]
- Siu LK, Yeh KM, Lin JC, et al. . Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis 2012;12:881–7. 10.1016/S1473-3099(12)70205-0 [PubMed] [CrossRef] [Google Scholar]
- Dubey D, Raza FS, Sawhney A, et al. . Klebsiella pneumoniae Renal Abscess Syndrome: A Rare Case with Metastatic Involvement of Lungs, Eye, and Brain. Case Rep Infect Dis 2013;2013 10.1155/2013/685346 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Kanoksil M, Jatapai A, Peacock SJ, et al. . Epidemiology, microbiology and mortality associated with community-acquired bacteremia in northeast Thailand: a multicenter surveillance study. PLoS One 2013;8:e54714 10.1371/journal.pone.0054714 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Korsten P, Vasko R, Gross O, et al. . Endophthalmitis, liver abscess, and cerebral and pulmonary emboli in a 48-year-old Vietnamese man. Internist 2014;55:722–5. 10.1007/s00108-014-3484-z [PubMed] [CrossRef] [Google Scholar]
- Sprenger K, Furrer H. Chameleons everywhere. BMJ Case Rep 2014. 10.1136/bcr-2014-205608 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Shah N, Owen L, Bhagani S. ‘Occam’s Scissors’: opportunistic infections in advanced HIV infection. BMJ Case Rep 2013;2013 10.1136/bcr-2013-009544 [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Saha I. Occam’s razor blunted. Trop Doct 2011;41:57–8. 10.1258/td.2010.100112 [PubMed] [CrossRef] [Google Scholar]
- Silber E, Sonnenberg P, Koornhof HJ, et al. . Dual infective pathology in patients with cryptococcal meningitis. Neurology 1998;51:1213–5. 10.1212/WNL.51.4.1213 [PubMed] [CrossRef] [Google Scholar]
- Ananworanich J, Chitwarakorn A, Wimonsate W, et al. . Hholtz T, and van Griensven F. HIV and Syphilis infection among men who have sex with men – Bangkok, Thailand 2005-2011. MMWR 2013;62:518–20. [PMC free article] [PubMed] [Google Scholar]
- Hung CC, Chang SY, Ji DD. Entamoeba histolytica infection in men who have sex with men. Lancet Infect Dis 2012;12:729–36. 10.1016/S1473-3099(12)70147-0 [PubMed] [CrossRef] [Google Scholar]
- Leung PO, Chen KH, Chen KL, et al. . Epidemiological features of intestinal infection with Entamoeba histolyticain Taiwan, 2002-2010. Travel Med Infect Dis 2014;12:673–9. 10.1016/j.tmaid.2014.04.010 [PubMed] [CrossRef] [Google Scholar]
- Leeyaphan C, Jiamton S, Prasertworonun N, et al. . Clinical and epidemiological characteristics of patients with syphilis: 5 year-case study from Thailand. J Med Assoc Thai 2014;97:963–8. [PubMed] [Google Scholar]
- World Health Organisation (WHO). Prevention and treatment of HIV and other sexually transmitted infections among men who have sex with men and transgender people: recommendations for a public health approach. Geneva: World Health Organization, 2011. http://www.who.int/hiv/pub/guidelines/msm_guidelines2011/en/(accessed 25 Jul 2016). [Google Scholar]
- World Health Organisation (WHO). Report on global sexually transmitted infection surveillance 2013. Geneva: World Health Organization, 2013. http://www.who.int/reproductivehealth/publications/rtis/stis-surveillance-2013/en/(accessed 25 Jul 2016). [Google Scholar]
- Abdollahi A, Saffar H, Saffar H, et al. . Is the evaluation of Entamoeba histolyticainfection in HIV-positive patients of any clinical significance? Acta Med Iran 2015;53:46–50. [PubMed] [Google Scholar]
Articles from BMJ Case Reports are provided here courtesy of BMJ Publishing Group

